Oral surgery makes a lot of patients nervous. That’s fair. Most of that anxiety comes from not knowing what to expect, not from the procedures themselves.
The surgeries covered here are among the most commonly performed in dental medicine. They have strong safety records, well-established outcomes, and for most patients, the recovery is significantly easier than the chronic pain they were living with before. What follows is the clinical picture you’d get from a real conversation with your surgeon: what each procedure actually involves, when it’s genuinely necessary, and what recovery depends on.
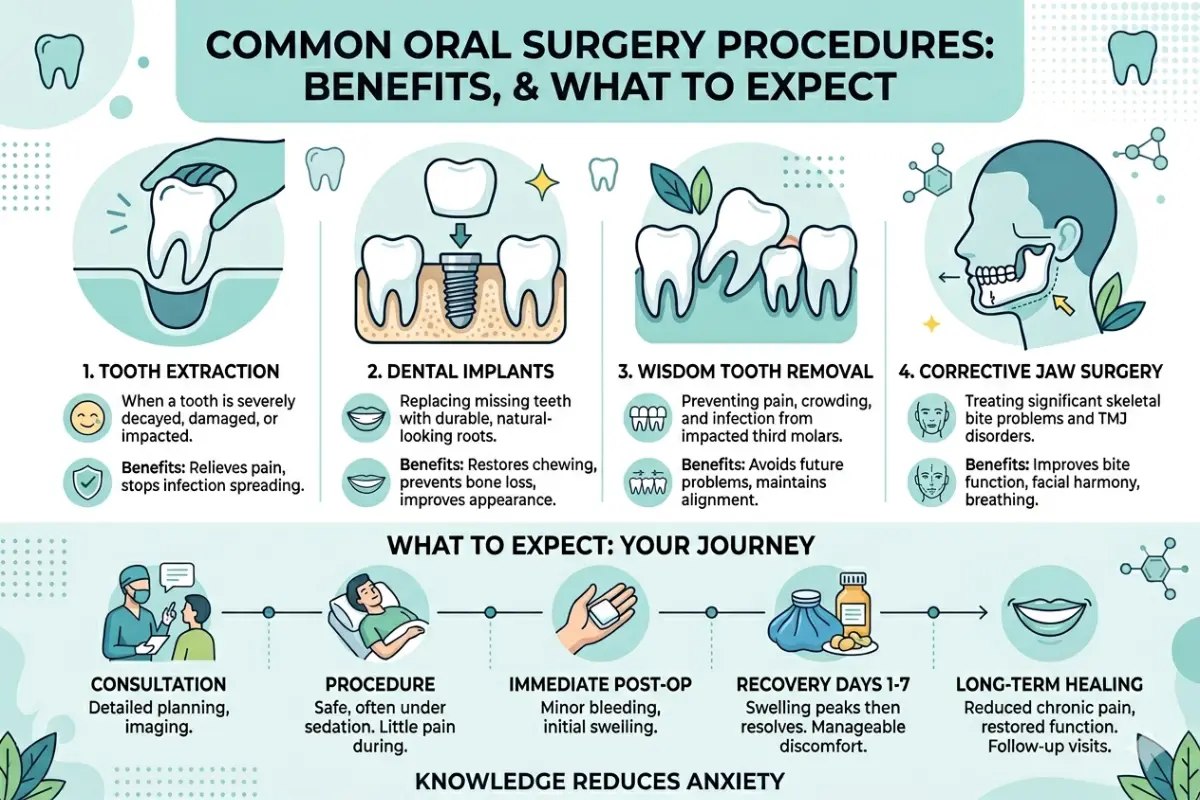
Tooth Extractions: When Removing a Tooth is the Right Call
Tooth extraction is the most commonly performed oral surgery procedure. In most cases, it’s a 30-60 minute appointment with a recovery measured in days.
Extraction is recommended when a tooth is too damaged or decayed to be saved with a crown or root canal, when infection has spread into the surrounding bone, when a tooth is fractured below the gumline, or when space is needed for orthodontic treatment. In every one of these cases, the goal is the same: stop the problem from spreading to adjacent teeth and bone.
A severely decayed tooth doesn’t automatically need extraction, though. If the root structure is intact and there’s adequate bone support, a root canal and crown is almost always the better long-term choice. The American Association of Endodontists is direct on this: saving a natural tooth is preferable to extraction when it’s feasible. The key variable isn’t how bad the decay looks — it’s whether the root and surrounding bone can support restoration.
The procedure itself is straightforward. Local anesthetic numbs the area completely. The tooth is loosened from the socket using an elevator instrument, then removed with forceps. For teeth that are broken or partially impacted, a small incision in the gum is needed first, that’s a surgical extraction rather than a simple one, and it adds some recovery time.
After extraction, a blood clot forms in the socket. That clot is the foundation for new tissue and bone to grow in. Protecting it in the first 72 hours, avoiding straws, smoking, and forceful rinsing, is the most important post-op instruction you’ll get.
One thing worth being clear about: the gap left by an extraction matters. Adjacent teeth gradually shift toward the space. The bone beneath starts to shrink within months. If you’re planning a replacement, timing the placement correctly is important.
Dental Implants: What Makes Them Work, and When They Don’t
A dental implant replaces the root of the missing tooth, not just the visible crown. A small titanium post is placed into the jawbone, where it fuses over 3-6 months in a process called osseointegration, the bone grows around and bonds to the titanium. Once integrated, it supports a crown that looks and functions like a natural tooth.
Implants have the best long-term outcomes of any tooth replacement option. They preserve the bone that would otherwise shrink after extraction. They don’t rely on adjacent teeth for support the way a bridge does. NIH research on implant survival rates puts 10-year success above 90% in healthy, non-smoking patients.
The most common reason a patient isn’t an immediate implant candidate is insufficient bone volume. The post needs at least 1mm of healthy bone on all sides to integrate successfully. Patients who’ve been missing teeth for years often have significant bone resorption, and the jaw has shrunk without a root to stimulate it. A bone graft is needed first, which adds months to the timeline but doesn’t change the eventual outcome. Working with an oral surgery provider in Cleburne ensures proper placement and long-term success. Implants are a durable and effective option.
Timing after extraction matters too. Same-day implant placement works well when the socket is healthy: good bone, no infection, intact socket walls. When the socket is infected or bone walls are compromised, AAOMS clinical guidance is clear that failure rates rise significantly. Delayed placement, waiting 3-6 months, gives the surgeon a more stable site and better long-term results.
For complex cases, standard 2D X-rays show bone height but not width or density. CBCT scanning gives a 3D map of bone dimensions. Research consistently shows it reduces surgical complications compared to planning from flat images alone.
Wisdom Tooth Removal: Who Actually Needs It and When
Wisdom teeth are the last to develop, usually erupting between the ages of 17 and 25. When they don’t have room to fully emerge, either partially erupting through the gum or remaining fully below the bone, they’re called impacted.
Impacted wisdom teeth can cause infection of the surrounding gum tissue (pericoronitis), pressure damage to adjacent second molars, cyst formation around the tooth crown, and chronic jaw pain. For patients in their late teens and early twenties with active impaction problems, removal is typically correct. Younger patients heal faster, roots are less developed, and surgical complexity is lower.
For older adults with asymptomatic, fully impacted teeth, the picture is different. Research published in the American Journal of Public Health found that many fully impacted teeth in adults over 25 remain stable and never cause clinical problems. If there’s no active pathology and the tooth is fully encased in bone, watchful monitoring is a defensible approach. The decision comes down to weighing real surgical risk against uncertain future risk.
The procedure involves a local anesthetic, a small gum incision, removal of any bone covering the tooth, and extraction, sometimes in sections for larger or awkwardly positioned teeth. Stitches dissolve over 7-10 days. Recovery for straightforward cases is typically 3-7 days.
Corrective Jaw Surgery: Functional Benefits Beyond Appearance
Corrective jaw surgery, orthognathic surgery, addresses structural problems with the jaw and bite that braces alone can’t fix. Primary candidates are patients who can’t chew normally, who have chronic jaw pain from misalignment, or who have airway restriction from jaw positioning.
The functional gains are real and lasting. Proper jaw alignment reduces strain on the temporomandibular joint, the jaw-to-skull joint, often resolving years of chronic headaches and facial pain. For patients with a significantly recessed lower jaw, it can improve airway clearance and, in some cases, resolve obstructive sleep apnea.
Surgery is always coordinated with orthodontic treatment. Braces align individual teeth within each arch before surgery. Surgery corrects the relationship between the arches. Post-surgical orthodontics fine-tunes the result. Full treatment typically takes 18-24 months.
AAOMS guidelines classify corrective jaw surgery as medically necessary when function is impaired, which is why many insurance plans cover a meaningful portion of the cost. The improvement in facial symmetry is a secondary benefit of correcting an underlying functional problem, not the reason to have it.
Gum Surgery for Advanced Periodontal Disease: What It Does and When You Need It
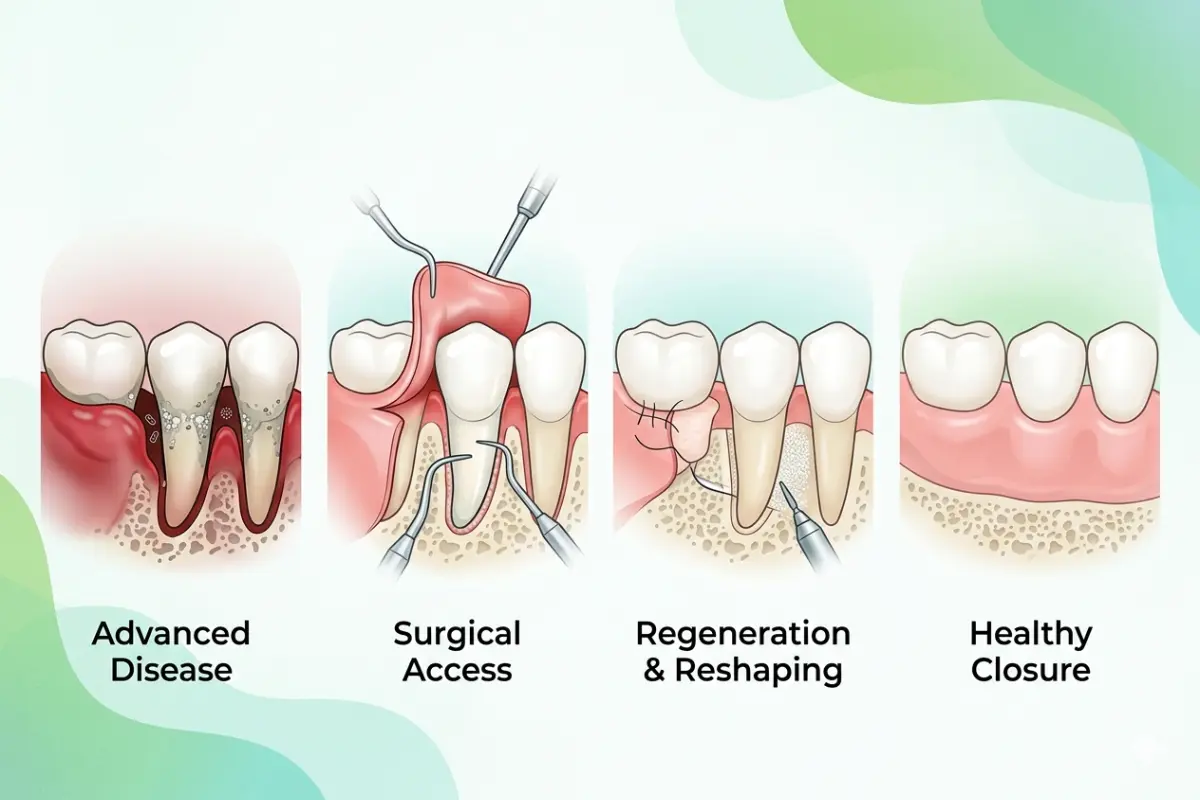
Gum surgery treats the structural damage caused by advanced periodontal disease, a bacterial infection of the tissues supporting the teeth. When pocket depths exceed 5-6mm and don’t respond to deep cleaning, surgery is the necessary next step.
The goal is threefold: remove infected tissue that deep cleaning can’t access, reshape the gum and bone architecture to eliminate the pockets where bacteria accumulate, and give the underlying bone the best chance to stabilize.
The most common procedures are flap surgery, lifting the gum tissue to clean root surfaces and underlying bone, and bone grafting, which replaces bone lost to disease. For patients with significant gum recession, soft tissue grafts restore the gum line and reduce tooth sensitivity.
Preventing tooth loss is the primary clinical benefit. Advanced untreated periodontal disease is the leading cause of tooth loss in adults. The American Academy of Periodontology is clear that surgery becomes necessary mainly when non-surgical scaling and root planing fail to reduce pocket depths after 4-6 weeks. If gum surgery is being recommended and you haven’t had a full course of deep cleaning first, that’s worth asking about.
Recovery is more manageable than most patients expect. Most return to normal activities within 2-3 days, with discomfort manageable with over-the-counter pain relief after the first 48 hours.
What Can Go Wrong: Managing Complications and Risk Factors
While serious complications from routine oral surgery are statistically rare, objective risk assessment is vital for true informed consent and proper postoperative management.
- Post-Surgical Infection
Occurs in approximately 1–5% of standard extractions. The risk increases for patients who are immunocompromised, have poorly controlled diabetes, or exhibit an active acute infection at the time of surgery. Clinical indicators of a secondary infection include a fever exceeding 101°F, visible purulent discharge at the surgical site, or asymmetric facial swelling that worsens after the third postoperative day. - Neurological Alterations (Nerve Injury)
The roots of lower third molars often sit close to the inferior alveolar nerve, which provides sensation to the lower lip, teeth, and chin. Temporary paresthesia (numbness or tingling) occurs in 0.9–5% of complex cases, while permanent nerve injury occurs in less than 1% of cases. Preoperative 3D CBCT imaging allows the surgeon to map this nerve relationship and adjust the surgical approach to protect it. - Medication-Related Risks and Bone Density
Patients taking antiresorptive medications (such as bisphosphonates or denosumab) for osteoporosis or oncology treatments face unique surgical risks. These medications slow bone turnover, which can lead to a condition known as Medication-Related Osteonecrosis of the Jaw (MRONJ), where the jawbone fails to heal after an invasive procedure. A thorough review of your medical history allows surgeons to implement specific protocols to protect the bone tissue.
Standard Post-Surgical Recovery Framework
This structured timeline applies to routine extractions and third molar removals. Actual recovery is governed by distinct biological and lifestyle variables, such as age, systemic stress, and nutritional optimization.
| Stage | Expected Clinical Presentation | Immediate Action Protocol | Clinical Red Flags |
|---|---|---|---|
| Day 0 (Surgical Window) | Persistent numbness; mild, controlled oozing; fatigue from anesthesia. | Maintain firm pressure on sterile gauze for 30–45 minutes; apply external ice packs (20 mins on/off); consume cool liquids and soft foods; rest with head elevated. | Heavy, continuous bleeding that fails to slow after direct pressure; inability to swallow liquids. |
| Days 1–2 (Inflammatory Phase) | Normal surgical soreness; facial swelling and bruising beginning to peak. | Continue soft-food diet; introduce warm compresses at the 48-hour mark; maintain gentle oral hygiene, avoiding the direct surgical sites. | A systemic fever exceeding 101°F (38.3°C); rapid, asymmetric swelling. |
| Days 3–5 (Vulnerable Clot Phase) | Swelling begins to decline; surgical soreness transitions to a dull ache. Risk window for alveolar osteitis (dry socket). | Initiate gentle warm salt-water rinses after meals (minimum 4–5 times daily); gradually reintroduce semi-soft foods; absolute avoidance of straws or smoking. | Sudden, severe, radiating pain accompanied by a foul taste or odor (indicative of dry socket). |
| Week 2+ (Tissue Maturation) | Soft tissue closure over the site; gradual return of normal jaw mobility and flexibility. | Transition back to a regular diet as comfort permits; attend your scheduled postoperative evaluation for suture assessment. | Persistent, localized numbness lasting past 14 days; swelling that returns unexpectedly after resolving. |
The Bottom Line On Oral Surgery
These procedures work. For the conditions they’re designed to treat, they consistently produce better long-term outcomes than managing problems that have progressed past what non-surgical care can fix.
Most complications are predictable and preventable. Most poor outcomes trace back to skipped imaging, missed medication history, or patients who weren’t given a realistic picture of what recovery involves.
Arrive at your consultation with specific questions: your surgeon’s case volume, what imaging will be used, and what recovery looks like for your age and health profile. The quality of those answers tells you a great deal about the quality of care you’ll receive.
About The Author:
Tany Clarck is a renowned blogger who specializes in the medical genre, especially in dental health. He has more than a thousand articles to his credit about perfect health. On numerous occasions, he has spoken about TMJ disorder, Oral hygiene, and similar mega trends related to dentists in Grand Prairie. In this article, he has researched the latest dental implant trends that are very popular in Fort Worth.
Medical disclaimer: This content is for informational purposes only and is not a substitute for professional medical advice.



